Authored by Roger Koops via The American Institute for Economic Research,
We have lost the meaning of “Land of the Free, Home of the Brave” to “Land of the Imprisoned, Home of the Afraid.”
2020 is a year of disguises. Some examples include computer models/modelers disguised as “science/scientists,” Tyrants/Dictators/Totalitarians disguised as “elected officials,” propaganda machines disguised as “news sources,” brainwashing disguised as “information,” censorship disguised as “public health safeguard,” panic and fear disguised as “social responsibility.”

Even the virus itself has been disguised by humans as an “apocalypse.” But, the last part is not the doing of the virus, but the doings of a select number of humans who are responsible for many of the other disguises as well. And if you look at the totality of events in 2020, it is clear that the average citizen has been treated generally less than human, certainly not as adults in any case.
I believe we are in as great a crisis as a species as we have ever been. The crisis is not from some seasonal virus (which is a health issue), but it is from ourselves and what we have devolved into as a species (social, cultural, ideological issues).
I have debated with myself on how to approach the following essay. Under normal circumstances, it would be easy. But, the topic has been so warped and sensationalized into political and social hyperbole, it is difficult to get a handle on it. I could go at it strictly from a scientific perspective, but that would tune many people out.
After about two weeks of my own internal debate and several versions, I have decided to treat the readers of this essay as Human Adults. I will try to not get too technical but rather use rational arguments to approach the issue of a viral infection from the perspective of the virus molecule outside of the host, i.e., the natural environment.
Computer modeling is “a” tool, not “the” tool. The model is only as good as the assumptions put into the model. It has been clear from the start that the modelers have NO idea of how a virus works in the natural world. They have based their modeling on the assumption that the culprit is the human being. The human being must be controlled in order to control the virus. This is completely wrong. I hope to present arguments that illustrate the weaknesses of the modeling concepts.
Human Perception
The natural perceptive abilities, i.e. the physical senses, of human beings are quite poor. For example, we can see only a very, very small part of the electromagnetic spectrum, illustrated as follows:

Consequently, humans have difficulty understanding that which is not directly observable by their senses. Size and mass we do okay at, providing we can see it. We tend to have better abilities with larger things that we can observe. But, even size perception has its limits. For example, many people cannot grasp the scope of our universe.
Smaller things, things we cannot see we have trouble with. We live, and have always lived, in a world with things that are far smaller than our ability to detect without some instrumental aid. For example, when I tell people that their bodies are mostly empty space, they scoff. We have solid substance, they say, we can feel it. I respond that the reason we feel it is solid is because that is how our brain interprets it.
For example, neutrinos are subatomic particles with no mass. They do not interact with matter. We are bombarded by interstellar neutrinos throughout our lives. They pass right through us. It makes no difference where you live because they pass right through the Earth, too. You can live a whole lifetime and never have experienced a collision of a neutrino with a cell in your body. Think about it; is it difficult to grasp?
Yes, neutrinos are exotic and basically of interest to physicists. But we exist in a constant interaction with other not-so-exotic things.
Bacteria and fungi, at the cellular level, exist at the micron scale (see the scale diagram below). But, they have the cellular machinery to grow on their own, i.e., their cells will divide and multiply as long as they have nutrients. We cannot see them normally without a microscope. But, if they keep growing, eventually we can see them (as things such as moldy bread, or mildew on the wall), or even feel them (old vegetables that get a “slimy” feeling actually have a bacterial plaque on their surface). Both bacteria and fungi can form “spores” to protect themselves under harsh conditions. It is a form of hibernation.
We have bacteria and fungi in our bodies constantly. Our immune system usually keeps them at bay, or more accurately, keeps them in balance. However, if our immune system weakens, or if a balance is shifted towards the bacteria/fungi, the balance can tip in their favor and we can experience disease. We tend to have more difficulty with control of bacterial/fungal infections than viral infections. In fact, the most common cause of a fatal outcome due to viral infection, including coronavirus, is a bacterial infection.
The reason the second week of infection is considered the worry stage is NOT because of the virus; rather this is the time when a weakened immune system, either by exposure or by losing the balance battle cannot prevent the bacteria/fungi from taking off. Most people who die from influenza, coronavirus, even rhinovirus, do so primarily from pneumonia (bacterial infection) or some other systemic bacterial infection.
Other things, besides fighting a virus, can weaken the immune system. Aging, diabetes/obesity, liver disease, kidney disease, cancer, lung disease, other infections (viral/bacterial/fungal), stress, circulatory problems, cardiovascular disease, and several others all can cause weakened immune systems (that is why they are called “comorbidities”). Clearly, the number and degree of conditions that weaken your immune system greatly increase the risk of severe disease or death from any infectious disease (bacterial, fungal, or viral).
All of these things occur at a level where our senses cannot perceive them. Fortunately, our bodies recognize these things at the molecular level and it is our own chemistry (we call “biochemistry”) that intervenes, mainly in the form of our immune system.
The Virus: What are we dealing with?
My Doctoral degree is in “organic” chemistry, specifically, chemistry involving carbon-based compounds. Chemistry is about working with problems at a molecular level. Guess what a virus like coronavirus is? It is a complex organic molecule. Organic chemists would call it a “macromolecule” where “macro” means large. It is only considered “large” in comparison to small molecules. I am naturally inclined to look at a virus like coronavirus as an organic molecule.
Coronavirus (CV) and influenza (IF) are very similar at the molecular level. Both are ribonucleic acid (RNA) viruses and both are enveloped helical (meaning that they have a similar 3- dimensional structure with a protein outer part and the RNA inside). CV is a positive strand RNA and IF is a negative strand RNA. This means they have opposite structures much like you have a left hand and a right hand. Their viral class identification is different partly for that reason.
Both CV and IF behave almost the same outside of the body and this is due to their size, structure, and relative chemical similarities. On average, both are about the same size, ranging around 100 ±30 nanometers or nm (CV can range smaller in size than IF). For consistency purposes, I will refer to both of them at the 100 nm size, which is reasonably accurate (nm is 10-9 meter (0.000000001 meter), a micron (μm) is 10-6 meter (0.000001 meter). The meter is about 10% longer than a yard, or 39.37 inches so 1 micron is 0.00003937 inch.
I have created the following scale for a reference point using font sizes, and I hope that the fonts are reasonably accurate. Note that our eyes cannot see 5 micron, so this is enhanced.
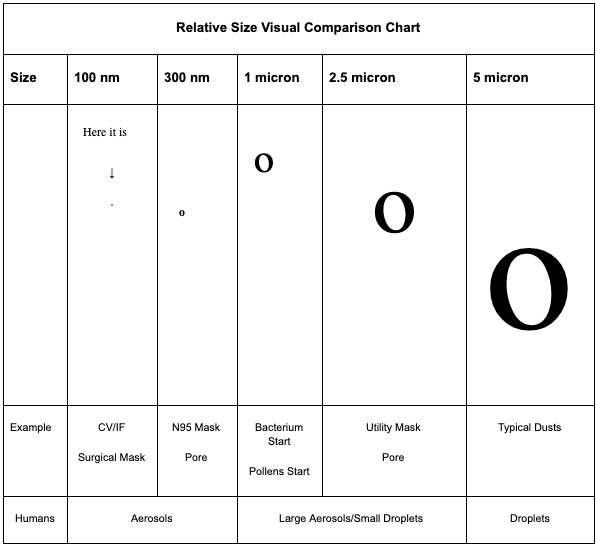
As the chart shows, both CV and IF as a molecule outside of the body are VERY, VERY small. They are undetectable without the use of an electron microscope. We simply cannot detect it in the natural environment. The tip of your finger, maybe 1 square millimeter, can literally pick up tens of millions of virus particles and you could not see any of them.
Because of the small size, we really do not know how they truly exist in the environment. They could be floating around as individual molecules, i.e. as single CV/IF particles. They could “aggregate,” meaning that they form clumps of molecules (again, too small to detect). They could attach to any other particle in the environment. Since they are so small, they could hitch rides with dust particles, pollens, leaves, just about anything that they may have an affinity for. The list of possibilities extends to anything you could think of in the environment, including living creatures. In short, they simply could be anywhere and everywhere.
Molecules can react with other molecules (reactivity), or they can remain as they are or fall apart into smaller molecules (stability). For the purpose of this essay, I will focus mainly on stability.
Most molecules have conditions that can render them either more stable or less stable. Clearly, with an infectious disease molecule, we would want to try and break it apart, or not give it stability. Breaking it apart usually renders it inert; i.e. non-infectious.
In an outdoor environment, we know that the CV/IF molecule will start to break apart within minutes or maybe last an hour or two. The local environmental conditions will determine how fast the molecule breaks up. We know that heat and ultraviolet (UV) radiation are pretty good at breaking it up.
There are things that chemically will help break it up. For example, saline conditions, like in an ocean are good (it may be considered a “natural disinfectant”). There are man-made disinfectants such as bleach. We know that CV/IF are not stable under pH of 3 or over a pH of 10. So if the molecule encounters either natural or man-made conditions that deal with these pHs, the molecule will break up. Common soaps are good for breaking up the molecule. This is why there is the recommendation to wash with soap and water.
Likewise, there are conditions that increase the stability of the molecule. Both CV/IF survive longer under colder conditions. This is probably one reason why they tend to favor winter months and colder climates.
We know that certain types of surfaces can make it more stable. For example, CV has good stability on plastic (1/2 life of almost 8 hours) and has even been detected up to one week on surgical masks. Some types of metals, such as copper, can speed up decomposition and some metals lend stability (such as stainless steel).
Skin can actually be good at destabilizing because of not only sweat but also the natural oils and detergents that are produced in the skin can break apart these types of molecules. That is a reason that skin absorption is not considered a vector of infection. Serious breaks in the skin, however, such as from burns or injuries, could lead to infection due to the decreased natural inhibition.
So, in general, we would want to try and increase exposure of the molecule to conditions that destabilize while trying to minimize the stabilizing conditions.
The Virus in Disease Transmission
The “rationale” for lockdowns, masks, distancing, etc. all rest on the assumption that human direct transmission is the greatest risk for disease. Anyone, at any given time, in any place can pass the virus to another. It sort of reminds me of the character “Cofi” in the movie “The Green Mile.” People seem to be convinced that somehow, the only way to catch this virus is because it makes a beeline from person to person. In other words, we are the culprits.
But, is this really the case? In short, “No” and here is why.
Because of the modeler’s view, if we imprison people (“lockdown” – a term used in penal institutions when prisoners become unruly), cover their faces (“masking”), and keep them from doing what people do, i.e. socializing (“distancing”), we can stop the virus. This concept is what “wanna-be” dictators all over the world have embraced.
This is NONSENSE. Certainly, you can get infected that way but that is only one way of many ways. It may not even be the main way. It is “losing sight of the forest for the trees.”
To examine the path to infection more closely, let’s make the following assumptions (which you can see are more or less worst case assumptions):
- Assumption 1. A person has CV/IF and is shedding, i.e. releasing virus from their bodies. Further, let’s focus on the nasal/oral route for shedding as the only route, even though we know that the virus can be shed from feces.
- Assumption 2. All shed virus is infectious. This may sound like a strange assumption but we really do not know HOW infectious shedding viruses truly are. What is being shed could be combinations of fragmented virus and more intact virus. The reason it is not clear is because a main method that is used for identification of samples is PCR. PCR cannot tell whether what is being amplified is actually infectious or not.
When we exhale breath, speak, sing, laugh, cough, shout, sneeze, hiss, scoff, grunt, etc., air is expelled from our, mostly, upper respiratory tract. This air MAY or MAY NOT contain particles of moisture (mostly water). These moisture particles MAY or MAY NOT contain mucus, cellular debris, bacteria etc. from our respiratory tract. These moisture particles MAY or MAY NOT contain virus particles. In other words, there MAY be virus particles hitching a ride or there may be NONE.
There is no scientific evidence that when a person is infected that they are continually expelling virus, but that goes to a different essay. Please note, I am not referring to the playground use of the “spitball,” which is a massive collection of saliva, which may or may not contain any of the above. However, I think that we all can agree that amorous kissing when there is an infected person involved runs the highest risk of transmission. But this has more to do with direct contact. I want to deal with indirect routes of transmission.
The expelled moisture particles range in size from very, very small to much larger and for scientific purposes are divided typically into two categories: (1) aerosols, which are the very small particles usually below 1 micron, and (2) droplets, which are particles larger than 5 micron. The range between 1-5 micron is sometimes ambiguously defined either as an aerosol or a droplet but that is not really important for this discussion. You can see the whole range is involved.
Once expelled (egress) away from the nose/mouth, moisture particles will travel certain distances depending on their sizes. Larger droplets fall closer to the individual while aerosols can travel much farther or remain suspended. We have imaging techniques to see droplets using special high speed cameras, but we cannot visualize aerosols.
Clearly, independent virus particles that are NOT hitching rides are expelled as nanoparticles and go out into the environment. We cannot begin to see these. But, as nanoparticles, we should assume that they can remain air suspended for long periods of time and are taken up by the local air movement patterns.
Aerosols and droplets, after leaving the mouth/nose will quickly lose their moisture, i.e. the water base will evaporate. The smaller the particle, the quicker this will happen. With aerosols, it may be within a fraction of a second. Environmental conditions will also affect the timing. Warmer and dryer conditions will speed up evaporation while colder and more humid conditions will slow it down. Studies have indicated that under most normal temperature conditions, aerosols and droplets less than 100 micron in size evaporate before they hit the ground.
What happens to the hitchhiking virus? IT IS STILL THERE! It does not evaporate. It has lost its ride but it is still there.
What happens to it now? It can go anywhere, i.e. it can be dispersed just like the free molecule. It will last as long as it is stable. It can be carried by the wind (outdoors) or by air movements or HVAC (indoors). It can hitch a ride with other carrier things (outdoor examples such as above). It can land on surfaces, any surface, whether indoors or outdoors. Animals or even insects can carry the molecule if it lands on them. If it lands on another person, it can land on their clothes, hair, skin, etc. and be carried by them. If it happens to get sucked into the respiratory tract or absorbed on the eye, it may eventually lead to infection if it can survive the body defenses. The possibilities really are endless.
Indoors, the picture becomes even more complicated because now the vectors of movement, displacement, and contamination possibilities increase. Air handling units can redistribute the molecules to other areas far from the original source. Surface contamination is now a real consideration. Simple items can become sources of infection.
For example desk pens and pencils, office equipment, telephones, notebooks, furniture, electronic devices, cups/glasses, dishes, light switches, etc. Just look around the room that you are sitting in and remember about when you (or someone) “dusts.” At least anywhere that a “dust” can go so can a molecule like a virus. In fact, the very act of “dusting” could reintroduce the molecule back into the environment. Anything in that environment that you touch is a potential source.
It should be easy to see why a lockdown is disastrous. A single sick person can spread a virus throughout a whole building and no one would know it until too late. Clearly, air handling, sanitation, people movement, shared items, all will play a significant role in transmission risk.
Further, indoor conditions are better generally for stability and survival of the molecule. Why are meat processing/packing plants at risk? They are refrigerated facilities. There are many people so there is a lot of movement. There are many surfaces for the molecule to sit, like carcasses, that are handled often and routinely.
I think people can start to see the problem that we are dealing with and why the virus doesn’t just go away so easily.
Don’t “Masks” Make A Difference?
Before going into that question, I want to provide both some personal background and maybe a little comic relief.
The photo below was taken about 30 years ago, and yes, that is me. I was being fit tested for my own respirator. In my first position after the Ph.D., I was given charge of developing a molecule that was so lethal (yes, it is used medicinally but in very dilute solutions and under strict controls) that even the tiniest of amount contacting my skin, nose, eyes, etc., could knock me out and kill without my ever knowing it; the risks I faced were far greater than any coronavirus. I had to undergo serious Personal Protective Equipment (PPE) training as a result. When your life hangs in the balance, you learn all that you can. I was also a member of an isolator design team to develop a manufacturing unit to contain the production process.

Yes, I do know something about PPE.
The type of respirator that I am wearing in the photo is designed to protect the wearer from chemical agents, mostly, although there are biological filters available. It has unidirectional airflow. That means that the air that I would breathe in would be pulled through a series of filter cartridges (the round canisters on the sides) in order to remove the potentially offending compounds. After inhalation, a valve would close off the incoming air (ingress) and my exhaled breath would exit via another one way valve (egress), which you cannot see but it is located in the middle of the canisters directly in front of my mouth. Of course, this was used with other head and body protection since ALL physical contamination had to be guarded against.
This kind of respirator required both fit and physical certification. I had to be certified on an annual basis to show that my lungs were capable of breathing with this apparatus since the pressure differential was great. That means, I had to be able to suck in the air through the filters as well as deliver out through the valve. Lung capacity was very important; it was NOT a normal breathing experience. You also had to take periodic breaks, as well as a thorough and careful decontamination after each use. The respirator worked only as long as the filter cartridges were effective. They could reach a saturation point or a point where the cartridge was spent and beyond that there would be no protection.
The idea of “masks” on people did not suddenly appear in March of 2020. The usage of face protection with infectious diseases has been well studied, especially with influenza. Do not forget, the mechanics of these two viruses (CV/IF) are essentially the same so what works or doesn’t work for one is the same for the other.
The understanding has been that a “mask,” and that term usually refers to either a SURGICAL mask or N95 mask, has no benefit in the general population and is only useful in controlled clinical settings. Further, it has been considered a greater transmission risk than a benefit in the general population. If people still have a memory, you may recall that this was still the advice in February 2020. That understanding has not changed and I will explain why.
The term “mask” by itself means nothing. It is like saying “car.” You have to identify it more specifically because there are many different types and varieties, just like cars. So, for this essay, I will use two terms as follows:
- Face Coverings: In this category I will include homemade cloth, dust, non-fitted utility, custom stylish, and any other common “mask,” i.e. something that is intended to cover your mouth and nose and that is by and large used in the general population (because they are cheap and inexpensive).
- Mask: In this category, I am referring specifically to the SURGICAL mask and N95 mask (which is recommended for use in clinical settings by health care workers). If necessary, I will specify between them.
One of the big mistakes by modelers is the concept of a face covering or mask as a “barrier.” I see many references to so-called “experts” who make this claim. This is completely false. No face covering or mask is a barrier. Either they do not know what they are talking about or they are misleading people.
Masks and “Face Coverings” ARE:
- FILTERS, not barriers. They FILTER only the things that they are designed to filter, to a level of efficiency based upon design, usually not at 100% efficiency. For example, the N95 mask is designed and rated to filter particles greater than 300 nm at 95% efficiency (note: there are masks with greater efficiency than 95%, such as the N99 and NHEPA, but these are very expensive).
- Bidirectional, or two-way street flow (unlike my respirator above). That means the air is intended to go in and out through the same place – breathe in, breathe out. The filtering ability affects both ingress and egress, but MOST are intended to be used towards ingress, i.e. to protect the wearer (Surgical masks are the exception).
- Designed for normal breathing patterns, not exertive force (although the Surgical mask has a pressure rating). This is an important point!
- NOT designed to filter infectious agents but rather inert particulates (except the Surgical mask which is intended to preserve a sterile/sanitary operating field).
- Designed for minimal usage time. They are NOT intended to be stuck on your face for hours.
I understand the psychological crutch that people feel with something covering their mouth/nose. I am sorry, but that is a false sense of security. Perception is NOT reality, just like the neutrino. The mind says that you have some solid thing covering your mouth and nose but that is not really the case, it is porous; things get through (or go around)..
I could spend time on the viral transmission ineffectiveness of the variety of face coverings and fitted masks based upon the material, pore size, non-fit, etc., as well as the studies. I will say that there has been only ONE type of mask, the SURGICAL mask, which has shown any ability to reduce, not eliminate, virus transmission because it is actually rated to a 100 nanometer pore size AND it is rated for ingress and egress. But, the SURGICAL mask is not intended for use outside of a controlled, sterile hospital surgical field where its use and function can be controlled. It has limitations.
In Part III above, the expulsion of the virus into the environment was examined. So, what happens if a person wears a mask/face covering? There are two different views of how the mask operates depending on whether it is ingress (protecting the wearer) or egress (protecting the environment). But, both add up to more or less the same thing.
First, what happens on EGRESS. We will look at droplets because most face coverings will not stop an aerosol and the 2020 propaganda has been focused on droplets.
Assuming that a person is shedding virus and they produce droplets that contain hitchhiking virus, and assuming the face covering actually stops ALL droplets (best-case scenario), the following molecular pathway will likely occur:
- The droplet will lose its moisture. The timing may be different than just going out into the environment but moisture will be lost. However, the expelled droplets may accumulate faster than evaporation. If that happens, the facial covering starts to become saturated with moisture, mucus, cellular debris, bacteria, etc. as well as virus molecules.
- The virus molecule DOES NOT EVAPORATE and no matter what happens as far as the droplet is concerned, the virus is now on the face covering, at least initially. This means that the face covering is now contaminated and is a possible source of transmission, both contact and airborne.
- The virus is not somehow magically “glued” to the mask but can be expelled, whether or not there is still moisture. This can happen the next time a person breathes, speaks, coughs, sneezes, hisses, grunts, etc. So, the virus can be expelled out INTO THE ENVIRONMENT from the face covering.
So, the face covering acts as an intermediary in transmission. It can alter the timing of the virus getting into the environment, but it now acts as a contact source and airborne source; virus can still get into the environment. Since we know that the stability is good on most covering and mask materials, it does nothing to break down the virus until the covering is removed and either washed or discarded (appropriately).
Here is an important point, as more virus molecules accumulate, more are expelled. The face covering is not some virus black hole that sucks the virus into oblivion.
Second, what about INGRESS?
What works for egress works for ingress. So, if a person is wearing a face covering and they encounter virus, aerosols, or droplets, the virus and aerosols will likely penetrate. If the droplet is stopped, the surface is now contaminated. This means that if the surface of the covering touches the mouth or nose, you can become contaminated, i.e. infected.
This is a common sight with most face coverings, including the “stylish” coverings that people are wearing (I often see the covering moving back and forth against their mouth and nose even as they breathe, like a diaphragm), as well as with the cheaper dust masks and homemade cloth masks. If you inhale, you can become contaminated. If you touch the face covering, such as pulling it up and down, you can become contaminated.
Further, because the surface is contaminated, a person can also expel the virus back out into the environment just as with egress. This can be done by talking, breathing, coughing, etc.
Stopping a *droplet* is NOT the same as stopping the virus!
This molecular evaluation only assumed the best case contact scenario; that is, 100% contact between the face covering and any virus particle that may be encountered. I have NOT examined low efficiency coverings, inappropriate use and handling, non-fit (air will circumvent the covering and go around it since air flow follows the path of least resistance – where the air goes so does a virus). I have NOT examined the eyes or ears as entry points. I have NOT examined the other modes of molecular movement on the surface of face coverings, such as osmosis. I have NOT examined the almost 100% misuse of any covering by the population at large simply because they have not been trained and have been misinformed and are using ineffective coverings.
It boggles my mind when there is some notion that by wearing a face covering you are actually doing a “service” to your neighbor and therefore everyone has to protect everyone by this. Actually, the opposite is true. You are now becoming an additional potential source of environmental contamination. You are now becoming a transmission risk; not only are you increasing your own risk but you are also increasing the risk to others.
To better illustrate, let’s look at my respirator above. If I had been exposed to the molecule that I described, the filters would have protected my breathing function (my other protective equipment such as gowns, hoods, etc. would protect the rest of me). But, the respirator surface would have been contaminated (as would the other gown surfaces). If I had gone out into an uncontrolled environment with that respirator (and/or gown, etc.), I could have released those molecules into the environment endangering any person, possibly fatally. I had to de-gown and decontaminate, very carefully, in a controlled environment to prevent that possibility. Even though I had been protected, I was still a risk to others.
Before March 2020, the standard Good Respiratory Practice (GRP) was to cover your mouth/nose when coughing or sneezing. It is especially effective if you use a tissue or handkerchief as a receptacle and cup your hand around them. The hand now actually DOES serve more as a barrier.
Plus, you will more likely remove the potential virus molecule from the environment by proper disposal of the tissue or washing the handkerchief. That is a practice we should be getting back to. I see people now who believe the misinformation and do nothing to shield their cough or sneeze because they believe that wearing a face covering is a barrier on its own. This is not good. So, at the very least, cover your face covering with your hands if you cough or sneeze!
I cannot tell people to not wear a face covering. I chose not to wear face coverings for two reasons, the first is all of the above, and the second is that I have experienced this virus. When I see people with them, I think of virus heaven. But, I am also not afraid because this virus does not frighten me.
I cannot tell people not to erect plastic sheets. But, when I see them, I see a virus motel-check in, stay a while, and then leave. This concerns me more because of the much larger surface area that can act as a virus repository. I have actually advised some places that have done this to either disinfect regularly, or move to glass where disinfection is easier. If there is virus stuck to these surfaces, there is both contact risk and expulsion risk back into the environment.
My view of dealing with the virus is at the molecular level. Do what we can to actually deplete the molecule, not give it stability.
We cannot eliminate this or any other upper respiratory virus. Maybe someday we can advance our immunological techniques to the point that it might be possible to make it a minor player in humans, but we are not there yet. But, we can defend against it by our immune systems and by trusting those with stronger immune systems to protect the weaker. Despite the propaganda, herd immunity was the standard before March 2020; it is not a “fringe” concept.
Here are some important points to consider:
- People who have experienced this virus do NOT need to wear face coverings, period.
- In the open environment, no one should be wearing face coverings. This is the one place where we can get an assist from nature to help reduce the virus molecules. Considering that less than 5% of transmissions have been associated with open environments (and identifiable activities not random encounters), the risk is truly small.
- A face covering may be useful when visiting an at-risk elderly person or in a controlled health care setting such as a hospital or nursing home. But, I think that these should be dispensed by trained personnel and should be focused on using Surgical masks wherever possible. The protection is not so much from viruses but face coverings may be more effective in preventing the spread of bacteria and fungi.
- Children should not be wearing face coverings. We all need constant interaction with our environments and that is especially true for children. This is how their immune system develops. They are the lowest of the low risk groups. Let them be kids and let them develop their immune systems..
- The “Mask Mandate” idea is a truly ridiculous, knee-jerk reaction and needs to be withdrawn and thrown in the waste bin of disastrous policy, along with lockdowns and school closures. You can vote for a person without blindly supporting all of their proposals!
- There may be other health risks associated with continued use of face coverings. While this is anecdotal, I have many physician acquaintances and they are all reporting increases in conditions that may be associated with face coverings, such as facial skin infections, nose/throat and sinus infections, even anxiety conditions. An area of concern is the change in breathing patterns that can be directly associated with face coverings. I train regularly. The only time that I wear a face covering is to gain entrance to the public gymnasium where I train (because it is required). The mask is discarded immediately when I start training, as most other people also do. The staff members do not make a fuss because they understand the dangers of doing exertion with a face covering.
- We also do not know enough about the possible consequences of forcing whole populations to adopt face coverings for extended periods. There may be both health and social consequences that we cannot consider at this time. Humans have developed as creatures whereby we interact with our environment. Our whole upper respiratory tract has developed immense defensive systems because of that. I am worried personally about “unnatural selection.” This is when human actions force a direction of evolution that would not otherwise occur. Often, the result is not good. But that is a whole different subject that needs to be considered.
I think that people can see how truly complex and difficult it is to deal with a nanoparticle. It is something too complex for modeling, at least on the environmental scale. It should be clear that humans are only a small part of the equation.
Stopping humans from being human will not stop the virus from being a virus!
We certainly should not have let modeling be experimented with on a worldwide scale directing policy that we had no idea of the outcome; but we did. It should be readily apparent by this time that all of the lockdowns, masking, distancing, closures, etc. have had no effect on the virus. It is time to reverse course.
Modeling could be useful in evaluating conditions in very limited and controlled settings. For example, it could be helpful to design infectious disease care units in hospitals. We could use modeling to examine our knowledge and use of air-handling, people movement and interactions in combination with molecule destruction, PPE, etc. to maybe develop better procedures to protect health care workers but also help reduce viral loads of patients.
For example, would a simply designed, single pass individual exhaust unit that carries the expired air from a patient to a chemical scrubber help reduce the viral load of the environment? Could it also help the patient by reducing the local viral and bacterial load? Could it help reduce or eliminate the molecule from those environments? These and others are questions that can be modeled and then tested. Then, maybe it can be tried on a pilot scale. If that works, maybe we can expand the scale, fine tuning as we go, and maybe reach a point where it works well and it can be used on a larger scale. That is how science works. Start small, gain understanding, finetune, and expand. You do NOT use the whole world as a laboratory on the first shot!
It is time for human beings to be human beings again. Stop trying to lay blame and guilt on people for a natural virus.
If governments want to be helpful in reducing severe disease and deaths, imposing more laws and restrictions is not the answer. Rather, focus on educating people on how to better maintain their immune systems. Encourage healthier lifestyles through education and wellness programs, especially in the less fortunate of our society. Provide or encourage businesses to consider better sick leave alternatives for people in ALL jobs/vocations so that people are not driven by the choice of work to live or stay home and be sick.
The healthy people in our society should not be punished for being healthy, which is exactly what lockdowns, distancing, mask mandates, etc. do. This goes completely against the principles on which the United States of America was founded. We have lost the meaning of “Land of the Free, Home of the Brave” to “Land of the Imprisoned, Home of the Afraid.”